Avian Influenza Bulletin – ‘tis the Season Reminder
From BCCDC:
 We are sending this pre-holiday bulletin as a reminder that the first three importations from China to North America of human infections with avian influenza (H5N1 and H7N9) were reported by Canada in early January 2014 (n=1) and 2015 (n=2), following the Christmas holiday period.
We are sending this pre-holiday bulletin as a reminder that the first three importations from China to North America of human infections with avian influenza (H5N1 and H7N9) were reported by Canada in early January 2014 (n=1) and 2015 (n=2), following the Christmas holiday period.
This includes a young adult from Alberta who acquired avian influenza A(H5N1) infection while in Beijing, China between December 6 and 27, 2013. Upon return to Canada, this patient was hospitalized with pneumonia, gastroenteritis and encephalitis and died in early January 2014. No poultry contact was identified while abroad. See: http://wwwnc.cdc.gov/eid/article/20/5/14-0164_article
In addition, a married couple from British Columbia acquired avian influenza A(H7N9) while traveling abroad in Hong Kong, Taiwan and Fujian province between December 29, 2014 and January 11, 2015. They recalled seeing live poultry and copious droppings while visiting Fujian on January 8, 2015 but recollected no other poultry contact. Both experienced typical influenza-like illness upon their return to Canada, and were managed as outpatients. Their avian influenza H7N9 infections were fortuitously recognized because of travel history and detection of non-subtypeable influenza A in respiratory specimens submitted to the BC Centre for Disease Control (BCCDC) Public Health Laboratory. See: http://wwwnc.cdc.gov/eid/article/22/1/15-1330_article
Recent Trends – H5N1 and H7N9
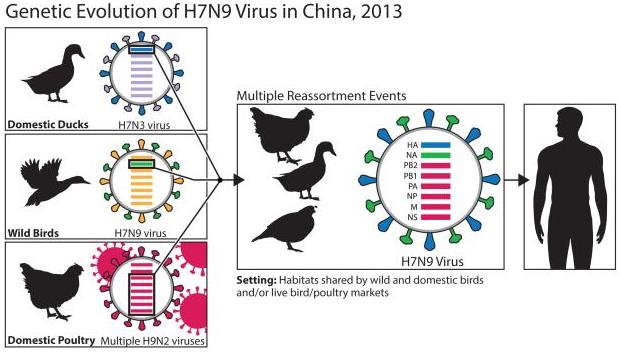
 Since its emergence in February 2013, H7N9 has followed a winter seasonal pattern, typical of both human and avian influenza viruses, with most cases occurring between October and May each year and generally peaking in January. A fourth wave of H7N9 activity appears to have recently begun in China, notably involving the eastern provinces of China as previously highlighted. Since October 2015, a total of 10 cases of H7N9 have been reported, including six new cases in the past week. These recent cases were reported in Zhejiang (5), Guangdong (1), Anhui (1), and Hunan (3) provinces, all of which have reported cases during the three previous seasonal waves. Overall, the epidemiological pattern of avian influenza H7N9 cases is unchanged from previous updates with older adults most affected (generally older than observed with H5N1). Exposure to poultry remains the major risk factor with only limited instances of human-to-human transmission in close contact settings. As of November 13, 2015, a total of 681 human cases of H7N9 and at least 275 deaths (case fatality: 40%) have been reported to the World Health Organization since first emergence in the human population in early 2013. This total does not include the six most recently reported cases (bringing the unofficial tally to 687 cases), but does include four cases reported from Taipei, 13 cases reported from Hong Kong, one case reported from Malaysia, and the two cases reported from Canada in January 2015 described above.
Since its emergence in February 2013, H7N9 has followed a winter seasonal pattern, typical of both human and avian influenza viruses, with most cases occurring between October and May each year and generally peaking in January. A fourth wave of H7N9 activity appears to have recently begun in China, notably involving the eastern provinces of China as previously highlighted. Since October 2015, a total of 10 cases of H7N9 have been reported, including six new cases in the past week. These recent cases were reported in Zhejiang (5), Guangdong (1), Anhui (1), and Hunan (3) provinces, all of which have reported cases during the three previous seasonal waves. Overall, the epidemiological pattern of avian influenza H7N9 cases is unchanged from previous updates with older adults most affected (generally older than observed with H5N1). Exposure to poultry remains the major risk factor with only limited instances of human-to-human transmission in close contact settings. As of November 13, 2015, a total of 681 human cases of H7N9 and at least 275 deaths (case fatality: 40%) have been reported to the World Health Organization since first emergence in the human population in early 2013. This total does not include the six most recently reported cases (bringing the unofficial tally to 687 cases), but does include four cases reported from Taipei, 13 cases reported from Hong Kong, one case reported from Malaysia, and the two cases reported from Canada in January 2015 described above.
Most H5N1 cases globally since 2010 (256/376; 68%) have been reported from Egypt, rather than China where
Action and Advice
Clinicians should remain vigilant for importation of suspect human cases of avian influenza to Canada, querying patients with acute respiratory illness, particularly if accompanied by severe or unusual features, about possible travel in the two weeks prior to illness onset. Where the index of suspicion is raised, clinicians should notify their local health authority/Medical Health Officer without delay and consult a virologist or microbiologist at the BC Centre for Disease Control Public Health Laboratory for advice related to diagnostic testing, clearly indicating relevant travel or exposure history. Follow strict infection prevention and control guidelines when collecting respiratory specimens.
Cases should be managed in respiratory isolation with contact and droplet precautions. Airborne precautions are warranted in the event of aerosol-generating procedures or conditions. Facilities should be mindful of the protection of other patients and visitors, in addition to healthcare workers, to minimize nosocomial transmission and risk.
Additional Resources
H5N1 Case Reports by Country and Year: http://www.who.int/influenza/human_animal_interface/EN_GIP_20151113cumulativeNumberH5N1cases.pdf?ua=1
H7N9 Case Definition – www.phac-aspc.gc.ca/eri-ire/h7n9/case-definition-cas-eng.php
ERV/SARI Case Report Form – www.phac-aspc.gc.ca/eri-ire/coronavirus/form-formulaire-eng.php
Case Management Guidelines – www.phac-aspc.gc.ca/eri-ire/h7n9/guidance-directives/h7n9-2-eng.php
Interim Antiviral Treatment Guidelines – www.ammi.ca/guidelines/